What Is a FUPA? Meaning, Causes, and How to Lose Pubic Fat
FUPA — or fatty upper pubic area — is common, normal, and widely misunderstood. Here's what causes it, why it lingers, and what actually works to reduce it.

*Disclaimer: We may earn a commission if you make a purchase through our affiliate links, at no extra cost to you.
📋 Quick Facts
Full Term
Fatty Upper Pubic Area
Fat Type
Subcutaneous & Mons Pubis Fat
Most Affected
Women (all body types)
Primary Causes
Weight gain, pregnancy, genetics
Can Be Reduced By
Diet, exercise, caloric deficit
Medical Procedure Option
Liposuction / Monsplasty
Spot Reduction Possible?
No — overall fat loss required
Medical Status
Normal anatomical variation
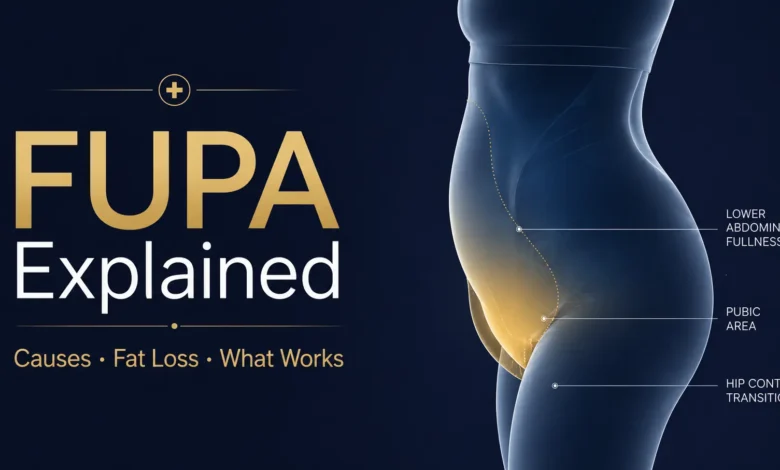
A FUPA — which stands for fatty upper pubic area — refers to the accumulation of fat tissue just above the pubic bone, in the region known anatomically as the mons pubis. It’s one of the most common and least discussed body concerns, affecting people of all sizes, ages, and fitness levels. The term itself entered popular usage through social media and colloquial health discussions, though the underlying anatomy has always been there. For those searching for what a FUPA is, the short answer is this: it’s subcutaneous fat that sits in the lower abdominal and pubic region, and for many people — particularly women — it’s simply part of how the body stores fat.
Understanding why this area collects fat, and what can realistically be done about it, requires separating fact from the noise of quick-fix advice that floods search results. The pubic area is biologically predisposed to fat retention, particularly in women, due to hormonal influences and the structural role of the mons pubis. Pregnancy, significant weight fluctuations, ageing, and genetics all contribute — none of which respond well to the kind of targeted “melt it in five days” promises that circulate online.
This guide draws on established exercise physiology, dietary science, and dermatological research to give an honest, grounded account of the FUPA meaning, what causes it, how to approach losing groin fat, and what to expect from both lifestyle changes and, where relevant, medical options. There’s no shortcut worth selling here — but there is a clear, evidence-informed path forward.
What Is a FUPA? Understanding the Anatomy
The mons pubis is a rounded mound of fatty tissue that sits over the pubic symphysis — the joint connecting the two halves of the pelvis. In women, this structure serves a protective and cushioning function, and its size is largely determined by genetics and hormonal environment. When people refer to a FUPA, they’re describing the visual fullness or protrusion in this region, which can become more pronounced with weight gain, post-pregnancy changes, or the natural redistribution of fat that comes with ageing.
Adipose tissue in the pubic and lower abdominal region is primarily subcutaneous, meaning it sits beneath the skin rather than around the organs (visceral fat). While visceral fat carries greater metabolic health risk, subcutaneous fat — including pubic fat — is harder to lose through exercise and tends to be one of the last areas the body draws on during a caloric deficit. This is not a design flaw; it reflects the body’s hormonal hierarchy for fat storage, particularly oestrogen’s role in directing fat deposition toward the hips, thighs, and lower abdomen in those assigned female at birth.
For men, similar fat accumulation occurs but is less commonly discussed. Male pubic fat tends to be associated more directly with overall abdominal obesity, and the anatomical structure of the mons pubis is less pronounced, making the visual presentation slightly different. That said, the mechanics of reducing it are broadly the same regardless of sex: overall fat loss through sustained caloric deficit, supported by resistance and cardiovascular training.
Why the Pubic Area Is Particularly Stubborn
Fat cells in the lower abdominal and pubic region have a higher density of alpha-2 adrenergic receptors compared to beta receptors. In plain terms, this means those fat cells receive stronger signals to hold onto stored energy and weaker signals to release it during fat mobilisation. Research published in the American Journal of Physiology has documented this receptor imbalance as a key reason lower body fat — in both the pubic area and thighs — is metabolically resistant. The body preferentially burns fat from areas with more beta receptors (upper body, face) before getting to regions like the mons pubis.
Pregnancy compounds this further. The connective tissue and skin overlying the pubic area can stretch significantly during gestation, and postpartum fat redistribution doesn’t always reverse cleanly, especially following caesarean delivery, where scar tissue can create a shelf-like appearance above the pubic bone. This is sometimes called a “C-section pouch” and is distinct from pure fat accumulation — involving both fat and loose skin, which responds differently to exercise.
Timeline: How FUPA Develops and Changes
Puberty
Oestrogen triggers fat deposition around the hips, thighs, and mons pubis as part of normal sexual development. The pubic fat pad becomes anatomically prominent for the first time during this phase.
Adulthood — Weight Gain
As overall body fat increases through caloric surplus, sedentary behaviour, or hormonal changes, fat cells in the pubic region enlarge. The FUPA becomes more visually pronounced and may cause discomfort in fitted clothing.
Pregnancy & Postpartum
The body increases fat stores throughout pregnancy. Postpartum, hormonal shifts and the physical stretching of abdominal tissue mean the pubic area often retains volume even as weight normalises elsewhere.
Perimenopause & Menopause
Declining oestrogen levels alter fat distribution patterns, shifting storage toward the abdomen and lower pubic region. Many women notice increased pubic fat during this phase even without significant weight gain.
Significant Weight Loss
After major weight loss, residual fat or loose skin in the pubic area can remain even when other regions have slimmed considerably. This is where exercise alone tends to fall short and non-surgical or surgical options may be considered.
Active Reduction Phase
Through sustained caloric deficit, strength training, and cardiovascular exercise, overall body fat reduces gradually — and with time and consistency, the pubic region will respond. Most people see meaningful change over 3–6 months of consistent effort.
💜 Why This Matters
Body image concerns centred on the pubic area carry a particular weight because they’re rarely spoken about openly — unlike belly fat or arm fat, which have entire fitness industries dedicated to them. For many women, especially postpartum, the FUPA is a physical record of pregnancy, hormonal change, or simple ageing, and the cultural pressure to erase it entirely can be quietly damaging. Understanding the biology not only makes the goal of reducing pubic fat more realistic; it also makes the experience of having it considerably less isolating. The body is not failing — it is, in many cases, doing exactly what it was designed to do.
How to Get Rid of a FUPA: What Actually Works
There is no exercise that burns fat exclusively from the pubic area. Spot reduction — the idea that targeting a muscle group with exercise will shrink the fat layer above it — has been consistently refuted by research in exercise science. A widely cited 2013 study published in the Journal of Strength and Conditioning Research found no localised fat loss in areas trained with resistance exercise compared to untrained areas in the same subjects. The mechanism of fat loss is systemic: the body draws from its total fat stores in a genetically influenced pattern, and no amount of pubic-area crunches or targeted yoga will override that.
What does work is creating a sustained caloric deficit — consuming fewer calories than the body expends — which forces fat mobilisation from all stored sites over time. For most people, a deficit of 300–500 calories per day is sufficient to produce meaningful fat loss (roughly 0.5–1 lb per week) without triggering the hormonal responses that make deeper deficits counterproductive. Combined with progressive resistance training — which builds muscle, raises resting metabolic rate, and improves body composition — and regular cardiovascular exercise, this approach produces genuine, lasting change. The pubic region will respond; it just tends to respond later than the face, chest, and upper body.
Practical dietary strategies matter too. Reducing refined carbohydrate and added sugar intake helps manage insulin levels, which directly influences fat storage signalling. Prioritising protein (research from the American Journal of Clinical Nutrition suggests 1.6–2.2g per kg of bodyweight for those in a fat-loss phase) supports muscle retention during a deficit and improves satiety. Hydration, sleep quality, and stress management all affect cortisol levels — a hormone that actively promotes fat storage in the abdominal and lower pubic region when chronically elevated.
How to Lose Weight in the Pubic Area: Exercise Strategies
While no exercise targets the pubic fat pad directly, certain training protocols create conditions that accelerate overall fat loss and improve the appearance of the lower abdomen and groin area. Compound resistance movements — squats, deadlifts, hip hinges, and lunges — recruit the largest muscle groups in the lower body and generate significant metabolic demand. This matters because muscle tissue burns more calories at rest than fat tissue, meaning building lower-body muscle creates a compounding fat-loss effect over time. According to data from the American Council on Exercise, strength training sessions can elevate post-exercise metabolism for up to 38 hours depending on intensity and volume.
Cardiovascular training plays a complementary role. High-intensity interval training (HIIT) has been shown in multiple controlled trials — including a 2018 meta-analysis in the British Journal of Sports Medicine — to reduce total body fat more efficiently than steady-state cardio at equal time investment. For someone with specific interest in losing groin fat, HIIT three times per week combined with two to three resistance sessions and daily movement (walking targets ~7,000–10,000 steps) creates a well-rounded protocol that doesn’t require heroic time investment.
Core strengthening exercises — including planks, dead bugs, and reverse crunches — do not burn the fat overlying the mons pubis, but they strengthen the muscles beneath, which improves posture, reduces lower abdominal protrusion caused by anterior pelvic tilt, and contributes to a flatter overall silhouette. This distinction is important: a prominent lower belly and pubic area is sometimes exacerbated by muscle imbalance and postural issues rather than fat alone, and addressing those will produce visible results even before significant fat loss occurs. If you’re also working on nutrition-related lifestyle improvements, combining dietary changes with movement creates the most consistent results.
📊 Effectiveness of FUPA Reduction Methods (Evidence Weighting)
Note: Effectiveness ratings are relative and based on published exercise science literature. Results vary based on individual starting point, consistency, and hormonal factors. Not a medical recommendation.
“Fat distribution is largely determined by genetics and hormones — not willpower. The lower abdominal and pubic region is one of the last places the body chooses to mobilise fat, and understanding that timeline sets more realistic expectations than any quick-fix programme ever could.”
— AB Rehman, Health & Lifestyle Writer, based on exercise physiology literature
Medical and Non-Surgical Options
For those who have already achieved significant fat loss but find the pubic area unresponsive — particularly postpartum women dealing with both excess fat and loose skin — medical procedures offer more targeted solutions. Liposuction of the mons pubis is one of the most commonly performed body contouring procedures, involving the removal of subcutaneous fat through a thin cannula under local or general anaesthesia. Results are generally considered stable provided overall weight is maintained, though the procedure carries the standard risks of any surgical intervention, including bruising, numbness, swelling, and, rarely, contour irregularities.
Monsplasty (also called a pubic lift) addresses cases where excess skin — not just fat — is the primary concern. This is more commonly pursued after bariatric surgery or major weight loss, where the skin’s elasticity has been compromised and cannot contract back adequately with exercise. The procedure involves excising excess skin and, in some cases, repositioning the mons pubis relative to the pubic bone.
Non-surgical alternatives include CoolSculpting (cryolipolysis), which applies controlled cold to freeze and destroy fat cells, and radiofrequency treatments that aim to tighten overlying skin. The evidence base for these in the pubic region specifically is more limited than for larger treatment areas like the abdomen. According to the American Society of Plastic Surgeons, results from non-surgical fat reduction are typically more modest than surgical options and often require multiple sessions. Cost data for these procedures varies considerably by geography and provider and has not been standardised for this specific region; consulting a board-certified plastic surgeon or dermatologist is advisable before pursuing any intervention.
Where Things Stand Now
Awareness of the FUPA as a medical and aesthetic topic has grown considerably over the past decade, partly driven by the broader body positivity conversation and partly by more open discussion of postpartum body changes across social media. Search volume data from Google Trends shows consistent and growing interest in terms like “how to get rid of fupa,” “what is fupa,” and “how to lose weight in pubic area female,” indicating that a substantial audience is actively looking for credible information rather than reassurance.
The clinical picture has also evolved. Plastic surgeons and gynaecologists have become more forthcoming about monsplasty and pubic liposuction as genuine — not merely cosmetic — procedures, particularly for women experiencing functional discomfort such as skin irritation, difficulty with hygiene, or chafing related to excess pubic tissue. Pelvic floor physiotherapists increasingly address postpartum pubic fat and associated tissue changes as part of comprehensive postnatal recovery, normalising the topic within formal healthcare settings.
From a fitness and nutrition standpoint, the science hasn’t changed, but the communication has improved. Mainstream health publications and certified trainers have moved away from promising spot reduction and toward honest explanations of how fat loss works systemically. For anyone currently working on this concern, the most useful current understanding is this: consistent caloric deficit and structured exercise will reduce overall body fat including in the pubic area — it simply takes longer there than elsewhere, and that delay is biological, not personal. Tracking progress through measurements and clothing fit rather than the scale or visual inspection of a single body area tends to produce both better outcomes and better mental health through the process. Those also working on overall health and wellbeing will often find that broader lifestyle consistency accelerates results in stubborn fat areas.
✨ FUPA — At a Glance
Fat Type
Subcutaneous
Spot Reduction Works?
No — systemic loss required
Avg. Reduction Timeline
3–6 months consistent effort
Medical Options
Liposuction / Monsplasty
❓ Frequently Asked Questions
What does FUPA mean?
FUPA stands for fatty upper pubic area. It refers to the accumulation of fat tissue in the mons pubis region — the soft mound just above the pubic bone. The term is widely used colloquially to describe visible fullness or protrusion in this area, and it applies to people of all body types, genders, and sizes.
What is a FUPA caused by?
The primary causes are overall weight gain, pregnancy and postpartum changes, genetic fat distribution patterns, hormonal shifts (particularly declining oestrogen during perimenopause), and significant weight fluctuations. In some cases, anterior pelvic tilt — a postural issue — can make the area appear more prominent without additional fat being present.
How do you get rid of a FUPA?
The most evidence-supported approach is a sustained caloric deficit combined with regular resistance training and cardiovascular exercise. There is no way to target fat loss in this area specifically — overall body fat must decrease for pubic fat to reduce. This process takes time, typically 3–6 months of consistent effort to see meaningful changes. Medical options like liposuction or monsplasty exist for cases where lifestyle change alone is insufficient.
How to lose weight in the pubic area female?
Women looking to lose pubic fat should focus on creating a moderate caloric deficit (300–500 calories below maintenance), prioritising protein intake to preserve muscle mass, and combining strength training with cardio. Exercises like squats, deadlifts, and HIIT sessions accelerate overall fat loss. Core work (planks, dead bugs) improves posture, which can reduce the visual prominence of the lower abdomen even before fat loss occurs.
Can exercise alone get rid of pubic fat?
Exercise alone is unlikely to eliminate a FUPA without accompanying dietary changes, because fat loss requires a caloric deficit. Exercise contributes to that deficit and improves body composition, but without dietary adjustment, the calorie gap is often insufficient for meaningful fat loss. The combination of structured training and nutrition management consistently outperforms either approach in isolation, according to published meta-analyses in the field.
Is a FUPA permanent after pregnancy?
Not necessarily, but it may be more persistent than fat in other areas. Postpartum fat in the pubic region can reduce with sustained lifestyle changes, though the timeline varies. If a C-section was performed, scar tissue can create a shelf-like appearance that fat loss alone will not fully resolve — in those cases, consulting a pelvic floor physiotherapist or a plastic surgeon about scar tissue management may be appropriate.
Final Thoughts
The FUPA meaning has been searched millions of times — and yet most of the content responding to that search is either medically thin or subtly alarmist. Fat in the pubic area is normal. It’s anatomically functional. It responds to the same biological rules governing fat storage and loss everywhere else in the body, and it requires no special protocol beyond the fundamentals of any sensible fat-loss approach: eat in a moderate deficit, move with consistency, build muscle, and allow time for the process to work in its own order.
The question of how to lose groin fat or how to lose weight in the pubic area female audiences most commonly ask about is really a question about patience and consistency, not about finding the right targeted exercise. The body will eventually draw from the pubic fat pad — it’s one of the more stubborn areas, yes, but stubborn is not the same as permanent. The research on this is clear and has been for decades; what’s changed is simply the willingness to explain it plainly rather than package it into clickable promises.
For anyone currently in the middle of this process, measuring progress only by how the pubic area looks on a given day is a reliable way to feel discouraged. Track overall body measurements, strength gains, cardiovascular fitness improvements, and how clothing fits. Those are the metrics that reflect a body in genuine, productive change — and the pubic area, given enough time, will follow.
📚 Sources & References
- Ramírez-Campillo et al. — Spot Reduction Study, Journal of Strength and Conditioning Research, 2013
- Viana et al. — HIIT vs Moderate-Intensity Cardio for Fat Loss, British Journal of Sports Medicine, 2019
- Morton et al. — Dietary Protein and Fat Loss, American Journal of Clinical Nutrition, 2015
- American Society of Plastic Surgeons — Liposuction Procedure Guide
- American Council on Exercise — The Truth About Spot Reduction
All sources verified at time of publication. Links subject to change.
AB Rehman
Health & Lifestyle Writer
AB Rehman is a features and research writer covering health, lifestyle, and body science. His work focuses on separating verified fact from speculation, drawing on primary sources and peer-reviewed research to produce accurate, readable long-form content for general and specialist audiences. He does not hold medical credentials; all health content reflects editorial research, not personal clinical guidance.
⚠️ Editorial Disclaimer
This article is intended for informational purposes only and does not constitute medical advice. All facts have been sourced from publicly available research and institutional sources at the time of publication. Where data could not be independently verified, this has been clearly noted. Nothing in this article should be treated as a substitute for advice from a qualified healthcare professional. Readers with medical concerns about body composition, hormonal changes, or post-surgical recovery should consult a licensed physician or specialist.

